Module 6: The Lymphatic and Immune Systems
Lesson 5: The Immune Response against Pathogens
Đáp Ứng Miễn Dịch Chống Lại Tác Nhân
Medical Terminology: The Lymphatic and Immune Systems
active immunity
acute inflammation
adaptive immune response
afferent lymphatic vessels
antibody
antigen
antigen presentation
antigen processing
antigen receptor
antigenic determinant
B cells
barrier defenses
bone marrow
bronchus-associated lymphoid tissue (BALT)
central tolerance
chemokine
chronic inflammation
chyle
cisterna chyli
class switching
clonal anergy
clonal deletion
clonal expansion
clonal selection
clone
complement
constant region domain
cytokine
cytotoxic T cells (Tc)
delayed hypersensitivity
early induced immune response
effector T cells
efferent lymphatic vessels
erythroblastosis fetalis
fas ligand
Fc region
germinal centers
graft-versus-host disease
granzyme
heavy chain
helper T cells (Th)
high endothelial venules
histamine
IgA
IgD
IgE
IgG
IgM
immediate hypersensitivity
immune system
immunoglobulin
immunological memory
inflammation
innate immune response
interferons
light chain
lymph
lymph node
lymphatic capillaries
lymphatic system
lymphatic trunks
lymphocytes
lymphoid nodules
macrophage
macrophage oxidative metabolism
major histocompatibility complex (MHC)
mast cell
memory T cells
MHC class I
MHC class II
MHC polygeny
MHC polymorphism
monocyte
mucosa-associated lymphoid tissue (MALT)
naïve lymphocyte
natural killer cell (NK)
negative selection
neutralization
neutrophil
opsonization
passive immunity
pattern recognition receptor (PRR)
perforin
peripheral tolerance
phagocytosis
plasma cell
polyclonal response
positive selection
primary adaptive response
primary lymphoid organ
psychoneuroimmunology
regulatory T cells (Treg)
right lymphatic duct
secondary adaptive response
secondary lymphoid organs
sensitization
seroconversion
severe combined immunodeficiency disease (SCID)
spleen
T cell
T cell tolerance
T cell-dependent antigen
T cell-independent antigen
Th1 cells
Th2 cells
thoracic duct
thymocyte
thymus
tissue typing
tonsils
type I hypersensitivity
type II hypersensitivity
type III hypersensitivity
variable region domain
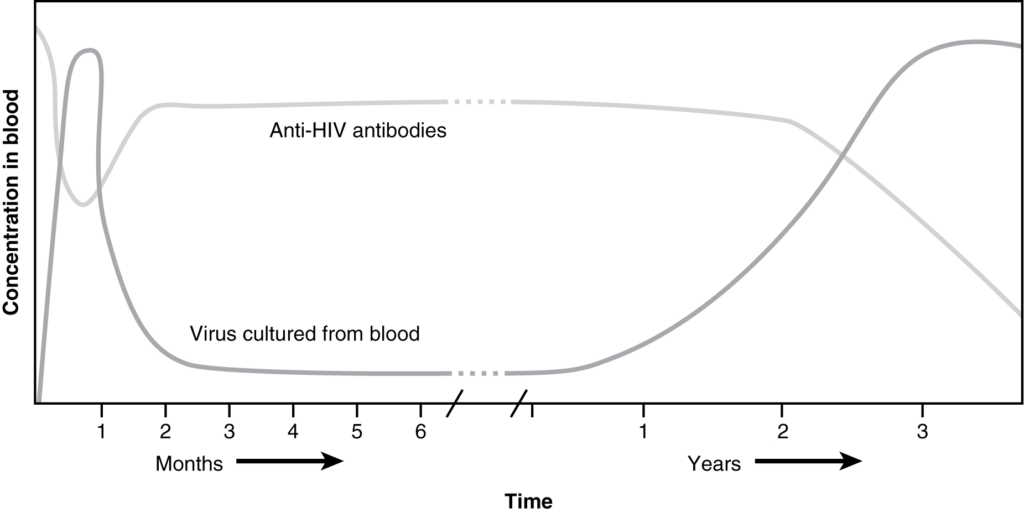
Seroconversion, the rise of anti-HIV antibody levels and the concomitant decline in measurable virus levels, happens during the first several months of HIV disease. Unfortunately, this antibody response is ineffective at controlling the disease, as seen by the progression of the disease towards AIDS, in which all adaptive immune responses are compromised.

LM × 40. (Micrograph provided by the Regents of the University of Michigan Medical School © 2012)
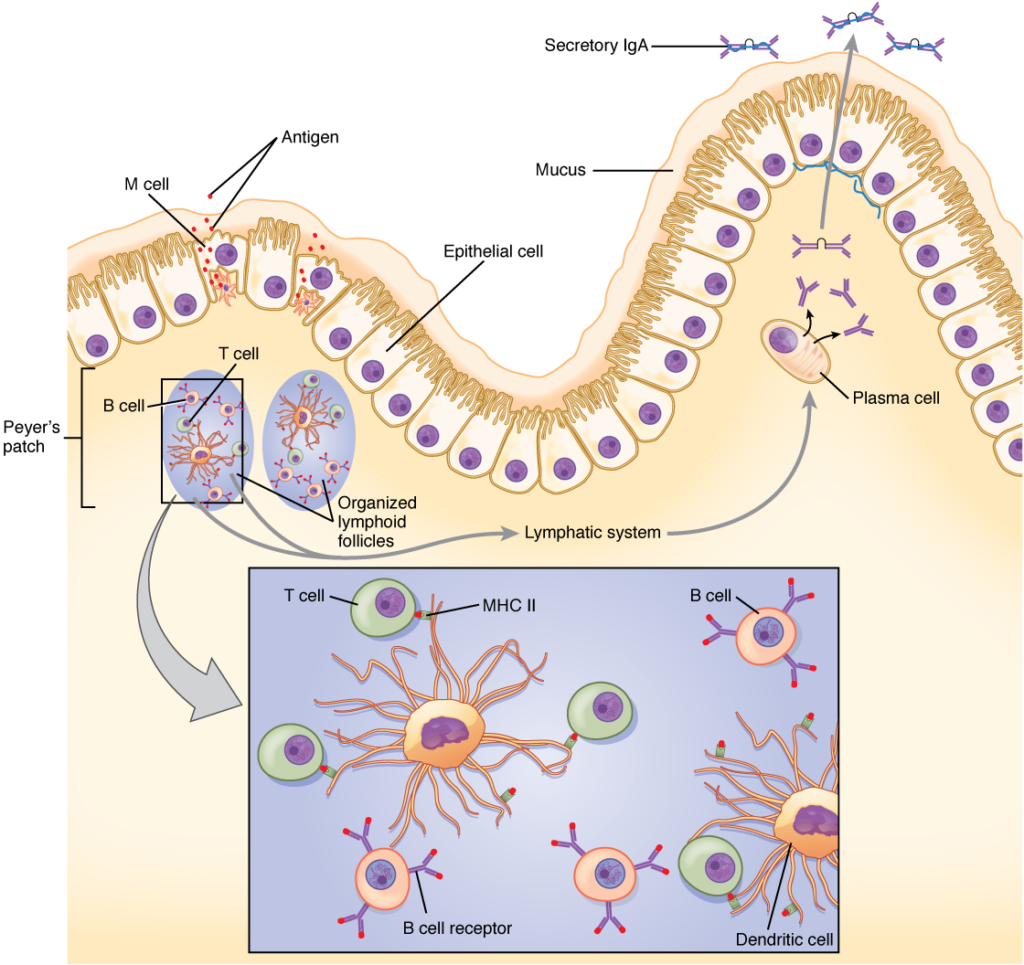
The nasal-associated lymphoid tissue and Peyer’s patches of the small intestine generate IgA immunity. Both use M cells to transport antigen inside the body so that immune responses can be mounted.
Ấn vào ô bên dưới để đánh dấu bạn đã hoàn thành bài học này
Quá dữ! Tiếp tục duy trì phong độ nhé!