Medical Terminology: The Neurological Exam
accommodation
accommodation–convergence reflex
anterograde amnesia
aphasia
ataxia
Babinski sign
cerebrocerebellum
check reflex
clasp-knife response
conduction aphasia
conductive hearing
conjugate gaze
convergence
coordination exam
cortico-ponto-cerebellar pathway
cranial nerve exam
cytoarchitecture
deep tendon reflex
diplopia
edema
embolus
episodic memory
expressive aphasia
extrinsic muscles of the tongue
fasciculation
fauces
fibrillation
flaccid paralysis
flaccidity
flocculonodular lobe
gait
gait exam
gnosis
graphesthesia
hemisection
hemorrhagic stroke
hyperflexia
hypotonicity
hypovolemia
inferior cerebellar peduncle (ICP)
inferior olive
internuclear ophthalmoplegia
intorsion
intrinsic muscles of the tongue
ischemic stroke
jaw-jerk reflex
localization of function
medial longitudinal fasciculus (MLF)
mental status exam
middle cerebellar peduncle (MCP)
motor exam
neurological exam
paramedian pontine reticular formation (PPRF)
paresis
plantar reflex
praxis
procedural memory
pronator drift
receptive aphasia
red nucleus
retrograde amnesia
Rinne test
Romberg test
rubrospinal tract
saccade
sensorineural hearing
sensory exam
short-term memory
Snellen chart
spasticity
spinocerebellar tract
spinocerebellum
stereognosis
stroke
superficial reflex
superior cerebellar peduncle (SCP)
transient ischemic attack (TIA)
vermis
vestibulo-ocular reflex (VOR)
vestibulocerebellum
Weber test
Wernicke’s area

The Snellen chart for visual acuity presents a limited number of Roman letters in lines of decreasing size. The line with letters that subtend 5 minutes of an arc from 20 feet represents the smallest letters that a person with normal acuity should be able to read at that distance. The different sizes of letters in the other lines represent rough approximations of what a person of normal acuity can read at different distances. For example, the line that represents 20/200 vision would have larger letters so that they are legible to the person with normal acuity at 200 feet.

The pituitary gland is located in the sella turcica of the sphenoid bone within the cranial floor, placing it immediately inferior to the optic chiasm. If the pituitary gland develops a tumor, it can press against the fibers crossing in the chiasm. Those fibers are conveying peripheral visual information to the opposite side of the brain, so the patient will experience “tunnel vision”—meaning that only the central visual field will be perceived.

Saccades are rapid, conjugate movements of the eyes to survey a complicated visual stimulus, or to follow a moving visual stimulus. This image represents the shifts in gaze typical of a person studying a face. Notice the concentration of gaze on the major features of the face and the large number of paths traced between the eyes or around the mouth.
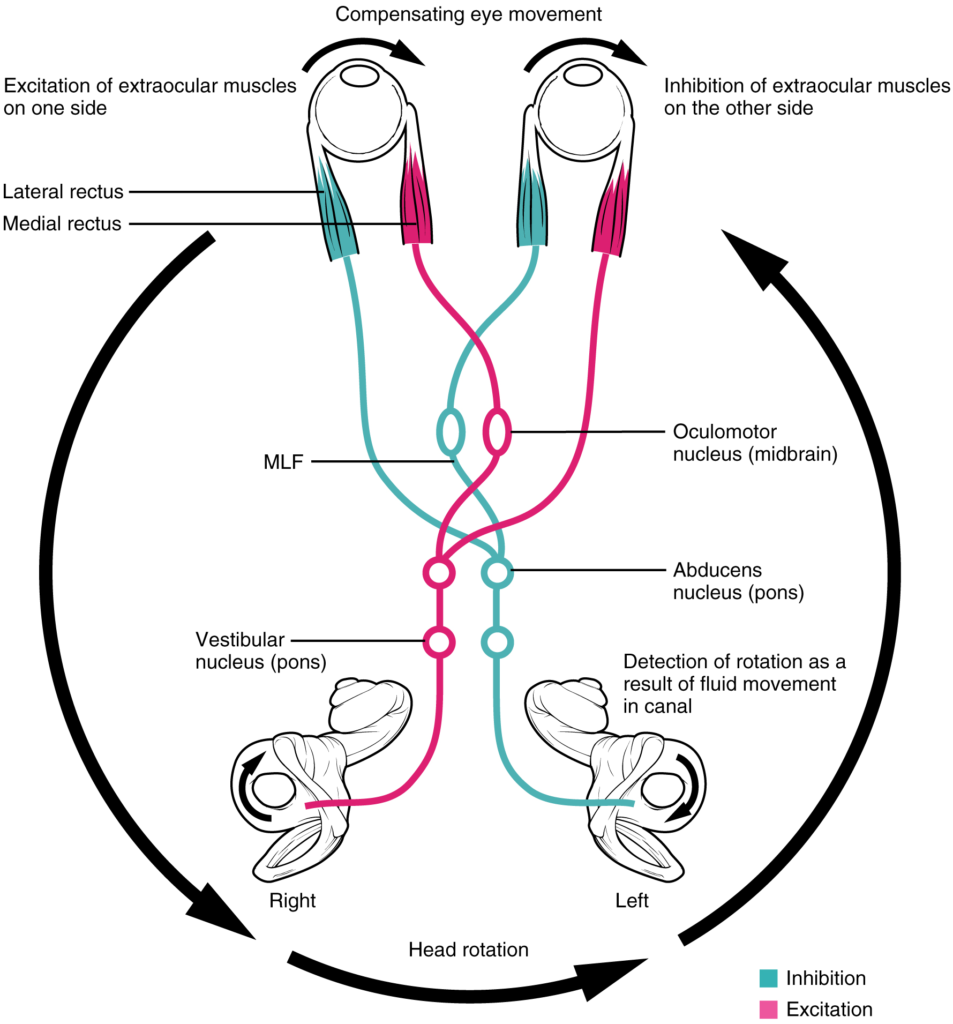
If the head is turned in one direction, the coordination of that movement with the fixation of the eyes on a visual stimulus involves a circuit that ties the vestibular sense with the eye movement nuclei through the MLF.

The accessory nerve innervates the sternocleidomastoid and trapezius muscles, both of which attach to the head and to the trunk and shoulders. They can act as antagonists in head flexion and extension, and as synergists in lateral flexion toward the shoulder.
Ấn vào ô bên dưới để đánh dấu bạn đã hoàn thành bài học này
Quá dữ! Tiếp tục duy trì phong độ nhé!