Medical Terminology: Joints
abduction
acetabular labrum
adduction
amphiarthrosis
annular ligament
anterior cruciate ligament
anterior talofibular ligament
articular capsule
articular cartilage
articular disc
articulation
atlanto-occipital joint
atlantoaxial joint
ball-and-socket joint
biaxial joint
bursa
calcaneofibular ligament
cartilaginous joint
circumduction
condyloid joint
coracohumeral ligament
deltoid ligament
depression
diarthrosis
dorsiflexion
elbow joint
elevation
eversion
extension
extrinsic ligament
femoropatellar joint
fibrous joint
fibular collateral ligament
flexion
fontanelles
glenohumeral joint
glenohumeral ligament
glenoid labrum
gomphosis
hinge joint
humeroradial joint
humeroulnar joint
hyperextension
hyperflexion
iliofemoral ligament
inferior rotation
interosseous membrane
intracapsular ligament
intrinsic ligament
inversion
ischiofemoral ligament
joint
joint cavity
joint interzone
lateral (external) rotation
lateral excursion
lateral flexion
lateral meniscus
lateral tibiofemoral joint
ligament
ligament of the head of the femur
medial (internal) rotation
medial excursion
medial meniscus
medial tibiofemoral joint
meniscus
multiaxial joint
opposition
patellar ligament
periodontal ligament
pivot joint
plane joint
plantar flexion
posterior cruciate ligament
posterior talofibular ligament
pronated position
pronation
protraction
proximal radioulnar joint
pubofemoral ligament
radial collateral ligament
reposition
retraction
rotation
rotator cuff
saddle joint
subacromial bursa
subcutaneous bursa
submuscular bursa
subscapular bursa
subtalar joint
subtendinous bursa
superior rotation
supinated position
supination
suture
symphysis
synarthrosis
synchondrosis
syndesmosis
synostosis
synovial fluid
synovial joint
synovial membrane
talocrural joint
temporomandibular joint (TMJ)
tendon
tendon sheath
tibial collateral ligament
ulnar collateral ligament
uniaxial joint
zygapophysial joints

An intervertebral disc unites the bodies of adjacent vertebrae within the vertebral column. Each disc allows for limited movement between the vertebrae and thus functionally forms an amphiarthrosis type of joint. Intervertebral discs are made of fibrocartilage and thereby structurally form a symphysis type of cartilaginous joint.
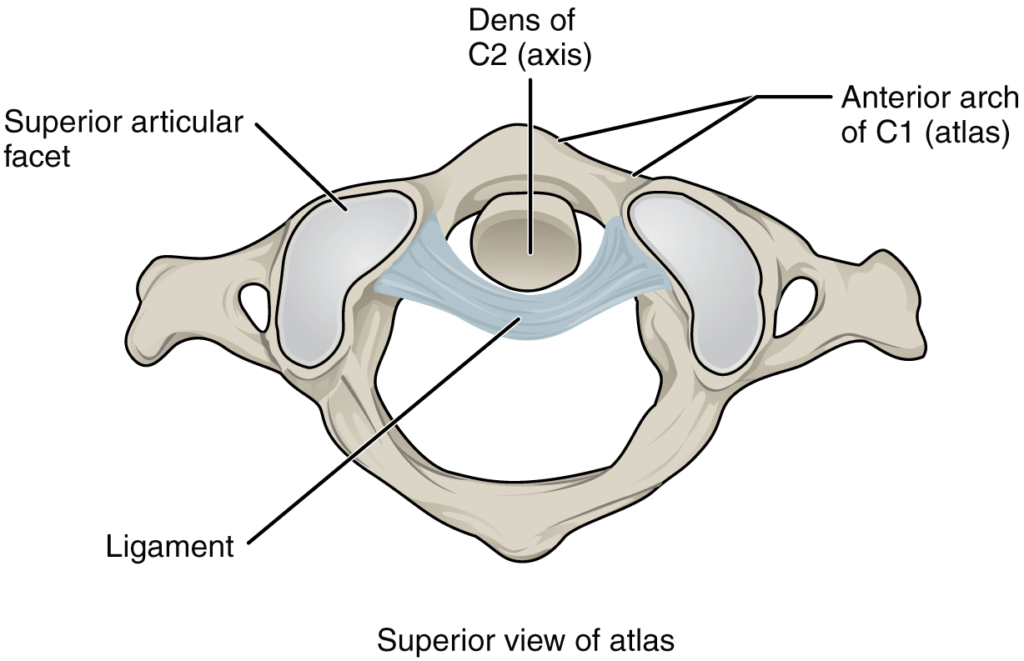
The atlantoaxial joint is a pivot type of joint between the dens portion of the axis (C2 vertebra) and the anterior arch of the atlas (C1 vertebra), with the dens held in place by a ligament.
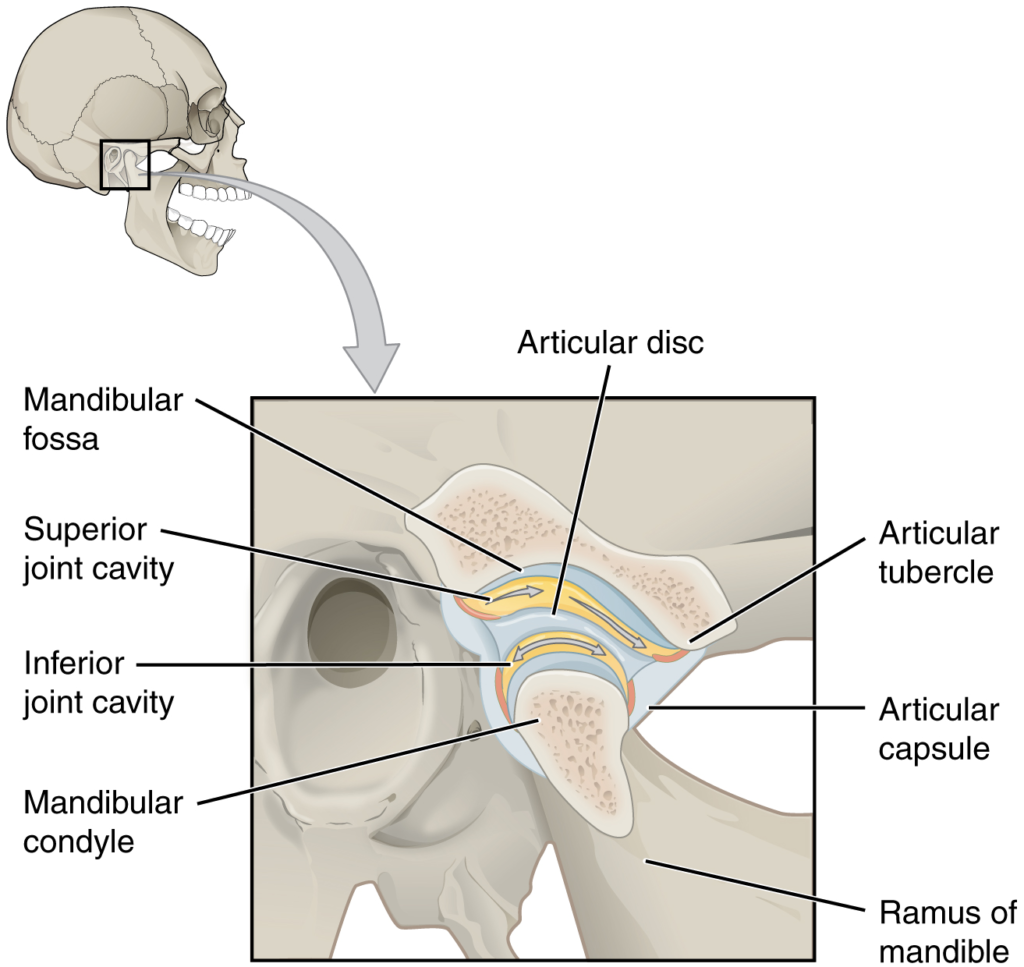
The temporomandibular joint is the articulation between the temporal bone of the skull and the condyle of the mandible, with an articular disc located between these bones. During depression of the mandible (opening of the mouth), the mandibular condyle moves both forward and hinges downward as it travels from the mandibular fossa onto the articular tubercle.
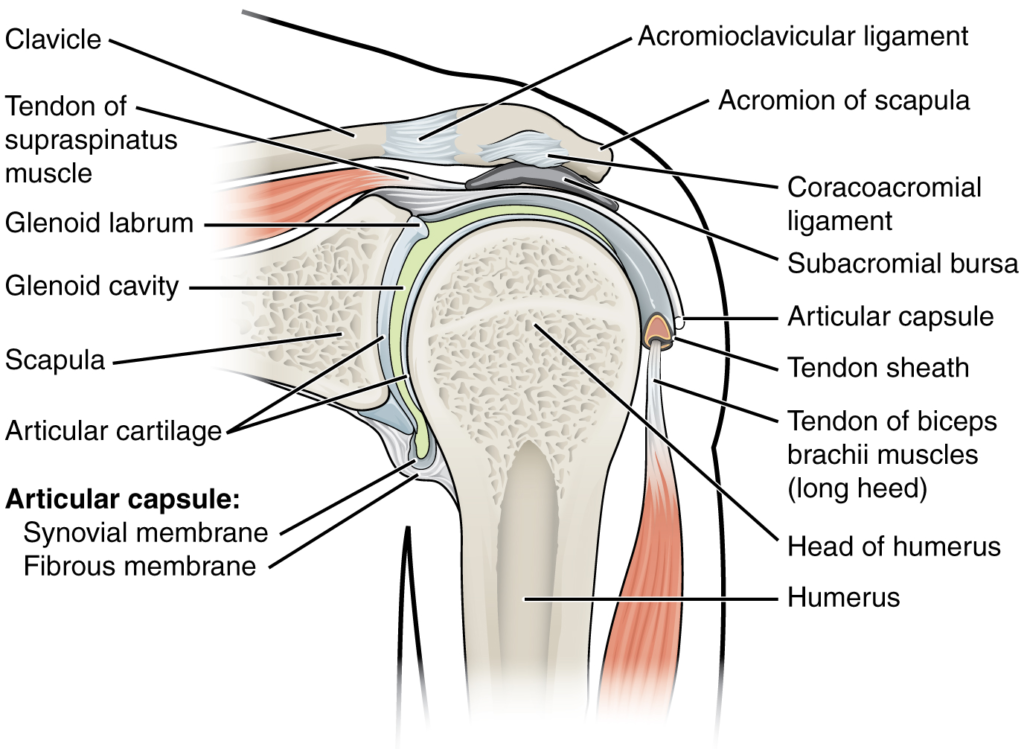
The glenohumeral (shoulder) joint is a ball-and-socket joint that provides the widest range of motions. It has a loose articular capsule and is supported by ligaments and the rotator cuff muscles.

(a) The elbow is a hinge joint that allows only for flexion and extension of the forearm. (b) It is supported by the ulnar and radial collateral ligaments. (c) The annular ligament supports the head of the radius at the proximal radioulnar joint, the pivot joint that allows for rotation of the radius.
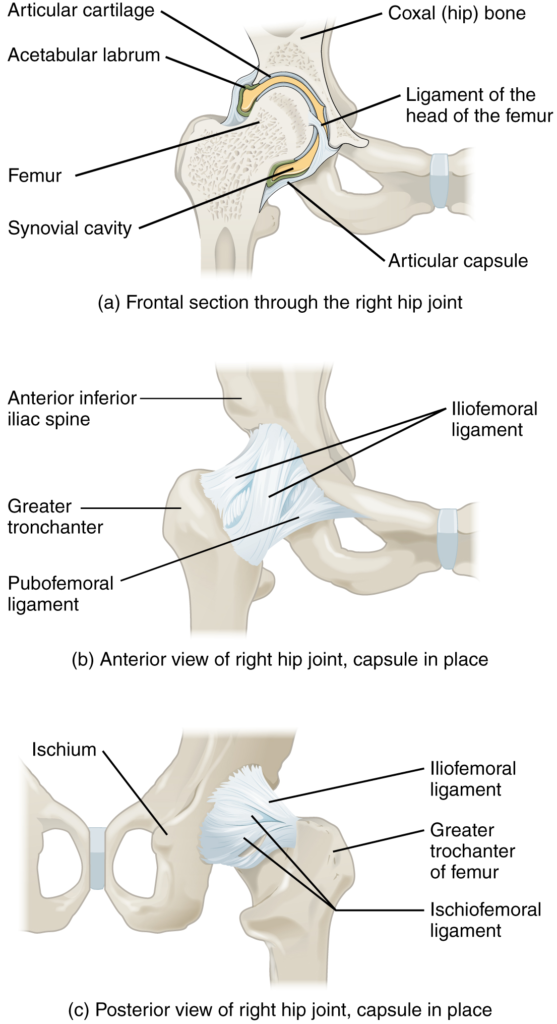
(a) The ball-and-socket joint of the hip is a multiaxial joint that provides both stability and a wide range of motion. (b–c) When standing, the supporting ligaments are tight, pulling the head of the femur into the acetabulum.
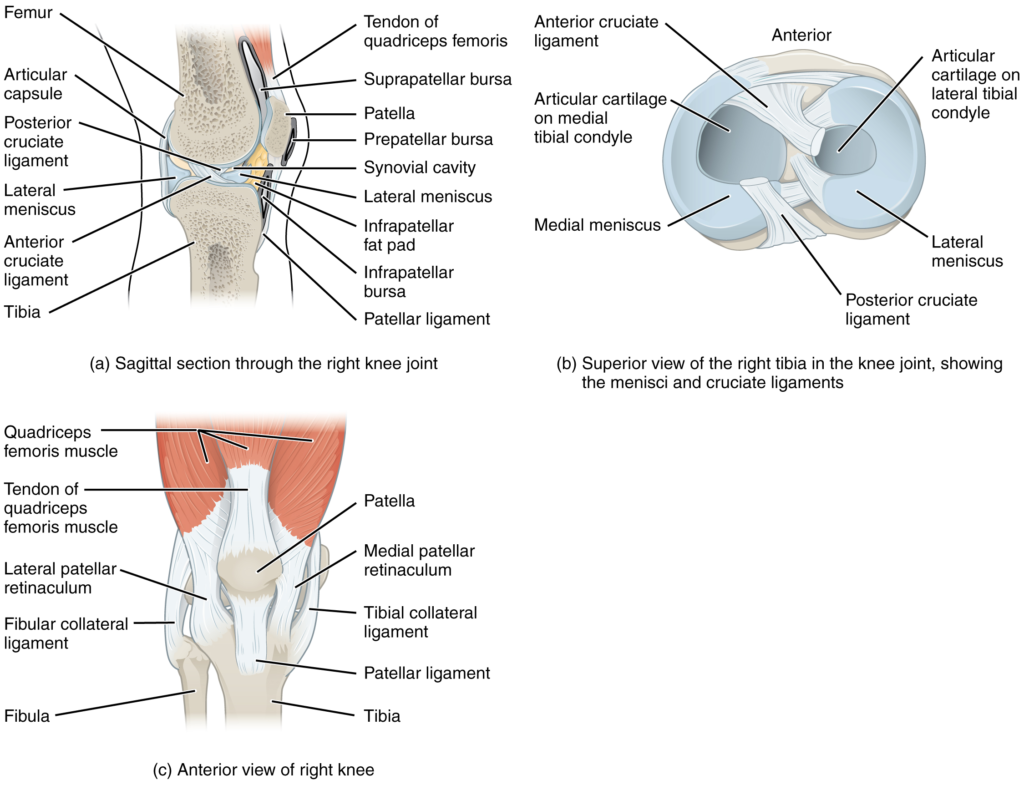
(a) The knee joint is the largest joint of the body. (b)–(c) It is supported by the tibial and fibular collateral ligaments located on the sides of the knee outside of the articular capsule, and the anterior and posterior cruciate ligaments found inside the capsule. The medial and lateral menisci provide padding and support between the femoral condyles and tibial condyles.
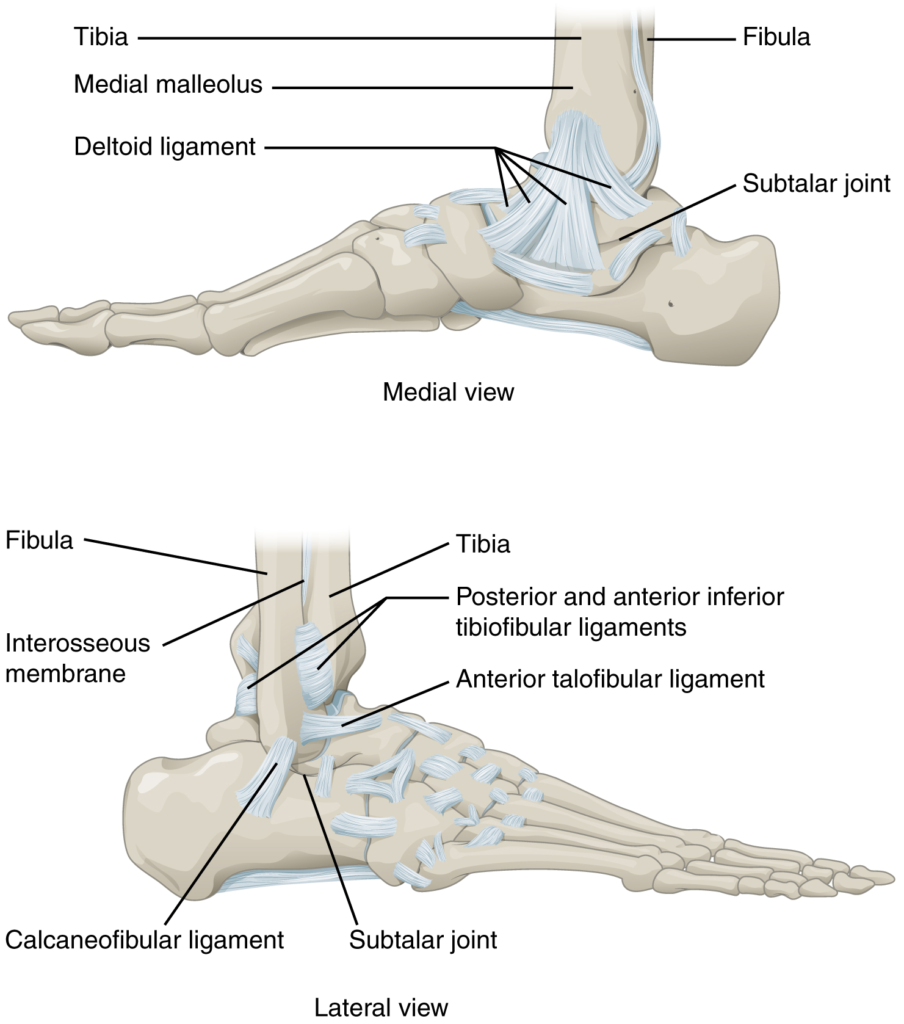
The talocrural (ankle) joint is a uniaxial hinge joint that only allows for dorsiflexion or plantar flexion of the foot. Movements at the subtalar joint, between the talus and calcaneus bones, combined with motions at other intertarsal joints, enables eversion/inversion movements of the foot. Ligaments that unite the medial or lateral malleolus with the talus and calcaneus bones serve to support the talocrural joint and to resist excess eversion or inversion of the foot.
Ấn vào ô bên dưới để đánh dấu bạn đã hoàn thành bài học này
Quá dữ! Tiếp tục duy trì phong độ nhé!